
Non-Operative and Alternative Treatments
Delaying or Preventing Hip Pain
Sometimes pain can be tolerated, but pain is usually a signal that something needs to be corrected rather than endured. When pain from hip dysplasia is severe, you should consult your doctor about definitive treatment by PAO surgery or a total hip replacement (THR). Ignoring pain too long as a young adult can cause more damage to your hip and eliminate the possibility of corrective surgery to restore your hip function.
The type of arthritis caused by hip dysplasia is called osteoarthritis. This means the smooth joint surface is wearing out like the tread of a tire wears out on a car. If the tire is out of balance, then the wear is faster than a well-balanced tire. Once the tread is gone, then it’s time to replace the tire. Tire treads often wear out with an uneven pattern and rotating the tires helps move the good tread into a better position so the tires last longer. For dysplastic hips it’s often possible to correct the imbalance with surgery and move the good cartilage into a better position to prolong the life of the hip surface and delay the onset of osteoarthritis.
When hip preservations surgery is not an option, there are a few steps you can take to help delay total hip replacement or to relieve pain until surgery is performed. Unfortunately, there aren’t any long-term cures for hip dysplasia other than surgical management.
Medications
Medications and cortisone injections can decrease the inflammatory component of your hip pain. Hip dysplasia causes swelling and irritation of the joint lining in addition to the pain from the thin joint surface or torn labrum. Medications may decrease the inflammation and help relieve pain, especially the nighttime pain that occurs when the hip is at rest. Some herbal remedies also act like medicines and these will be presented as Alternative Treatments.
If you have hip pain but do not currently need surgery, Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) include over-the-counter medicines like ibuprofen (Advil) and naproxyn (Aleve) can relieve inflammation and provide pain relief. While these medicines can provide short term relief, the anti-inflammatory effect may need three or four days of steady medication to have full effect. The instructions on the Aleve website say that you can take one or two tablets every 12 hours for a maximum of 10 days, but you should see a doctor if you plan to continue longer than that. There are also prescription anti-inflammatory medicines that your doctor can prescribe if you need more time or if you have side effects from over-the-counter medications. Your doctor can explain these medications to you and discuss recommended dosages.
Narcotic medications are not recommended for chronic hip pain because of the risk of dependency or addiction. This is especially true for hip dysplasia because current surgical techniques can produce long-term relief and return to activities.
Injections
Injections into the hip joint are often used to relieve pain and delay surgery. Recent developments include injections that may preserve or restore the hip cartilage. At this time, none of these techniques has been shown to provide long-term relief. While these advances may be useful for other causes of arthritis, there is little likelihood that people with hip dysplasia will benefit because the socket and ball will still be inadequate to support hip forces during walking.
Injections into the hip joint may be done by experienced physicians who are familiar with anatomical landmarks, but some physicians prefer to use ultrasound or fluoroscopy to guide the needle into the hip joint.
-
Cortisone Injections
These are the most commonly recommended injections to provide temporary relief that lasts from three to six months in most cases. Cortisone is a type of steroid that has strong anti-inflammatory effects. One problem is that multiple cortisone injections may soften the cartilage and increase the rate of deterioration. For that reason, most doctors try to avoid more than three hip injections of cortisone a year. There is a slight risk of infection with any injection but cortisone shots do not increase the risk of infection when a total hip replacement is eventually performed. However, it’s generally recommended to avoid cortisone shots in the months prior to total hip replacement surgery.
-
Hyaluronic Acid Injections
Hyaluronic Acid (HA) is a joint lubricant that’s found in normal joint fluid. Some benefits from HA injections have been reported for other joints, but hip joint studies have compared HA injections to cortisone injections. In almost all these studies, the cortisone injections gave better relief that lasted longer than HA injections.
-
Prolotherapy
Prolotherapy consists of injection of highly concentrated dextrose sugar water into a joint, tendon, or ligament to stimulate the healing process or to decrease pain. Platelet rich plasma or stem cells are occasionally added but generally, the sugar water alone is used. Prolotherapy causes inflammation that “jump starts” the healing process. This is thought to stimulate growth factors that are necessary for healing of ligaments, tendons and cartilage. Some success has been noted for tendon and ligament damage, and some studies of osteoarthritis have shown improvement in symptoms. No studies for labral tears have been published. Like other injections, prolotherapy does nothing to correct the underlying cause of joint deterioration from inadequate bone support of hip dysplasia.
-
Platelet Rich Plasma Injections
Platelet Rich Plasma (PRP) is a concentration of growth factors from a person’s whole blood. A sample of blood is taken and put into a centrifuge to isolate these growth factors and then the blood is returned to the patient while the PRP is injected into a site that needs additional stimulation. There is no evidence that this helps osteoarthritis caused by hip dysplasia. In one study PRP was used for patients undergoing arthroscopic labral repair but the authors found no benefit from this additional stimulation.
-
Stem Cell Injections
Bone Marrow Mesenchymal Stem Cells (BM-MSCs) are a person’s own bone marrow cells that can become into almost any type of cell including cartilage. These are concentrated from bone marrow and injected into the arthritic joint. Often three injections are performed one week apart. This is a generally safe procedure, but it is still experimental because results are questionable. There may be some benefit for joints with small segments of cartilage damage, but BM-MSC will not restore the bone alignment that causes arthritis from hip dysplasia.
Lifestyle Modifications
Lifestyle modifications can help delay surgery or recover from surgery. These include weight management, moderate exercise, adequate sleep, avoidance of harmful substances, stress management, proper nutrition, and heat therapy. Many books have been written about this subject, but here are some that may be specific to those with hip dysplasia.
-
Body Weight Management
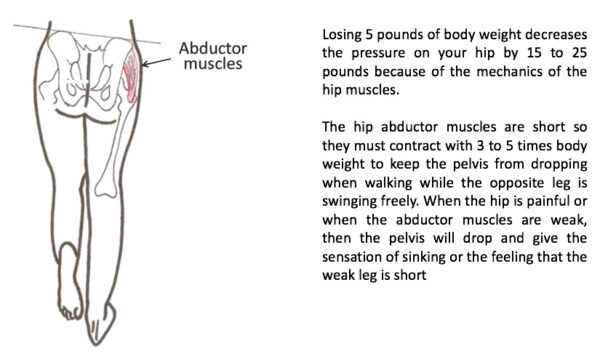
Losing a few pounds is the most beneficial lifestyle modification you can make. Even five pounds can damage the hip joint and make a big difference in comfort. The reason is that muscle leverage on the hip increases the force pressing the ball into the socket. One pound of body weight magnifies the joint pressure by three to five pounds. So, losing five pounds can decrease the painful forces by an equivalent of 15 to 25 pounds.
Another way to think about it is that body weight acts like a nutcracker and increases the pressure on your hip a lot more than you think because the hip joint is not directly under the center of your body. The hip muscles work hard to keep your pelvis level when walking. When your hip is in pain, the pelvis may dip so the pressure on the hip joint decreases.
-
Sports Activities and Exercise
Running, stair climbing, and impact sports are not recommended for people with hip dysplasia.
Moderate exercise and strengthening is preferred to maintain muscle balance long as there isn’t too much load put on the hip joint. Swimming is an excellent activity that maintains cardiovascular fitness and upper body strength in addition to low impact hip exercise. Other activities like rowing, cycling, or tennis may be possible in moderation, but these can be difficult for arthritic hips because of stiffness and stress across the hip joints. Sports like golf and bowling are unlikely to damage the hip but there may be pain in certain positions.
Movements of the hip and gentle stretching exercises are recommended because motion may help lubricate and nourish the joint surfaces. Tai Chi is excellent for flexibility and balance. Walking with a cane in the hand opposite the sore hip can also provide some physical activity in later stages of painful hip dysplasia.
Depending on the level of dysplasia, you may benefit from one or two visits with a local Physical Therapist to teach you the correct way to exercise without causing damage to your hip.
-
Adequate Sleep
This may be difficult if you’re having pain at night. Acetaminophen (Tylenol) is least likely to interfere with normal sleep patterns compared to NSAIDs such as aspirin, ibuprofen (Advil) or naproxen (Aleve). Regular bedtime with adequate time for sleep is important for repair processes and for stress relief. More time in bed may be needed along with an occasional daytime nap to make up for lost sleep due to pain.
Exposure to daytime light during the day and avoiding blue light prior to bedtime have been shown to help people fall asleep and have better sleep patterns. You can read about this in the Harvard Health Letter by clicking here. Computer screens, TV screens and hand-held digital devices emit blue light that can be decreased by adjusting some of these devices. Blue-blocking glasses, screen filters, and special light bulbs can also decrease blue-light exposure to help restore natural sleep patterns.
-
Avoidance of Harmful Substances
This applies most often to cessation of cigarette smoking. Any tobacco products or nicotine in any form, causes serious health consequences to your entire body including joints, ligaments, bones and muscles. Cigarette smokers have more complications after surgery than non-smokers. Cessation of smoking prior to surgery helps avoid complications, but the minimum time required isn’t known. At least two months seems to be the minimum in some studies, but longer is better, including no smoking after surgery too.
Alcohol in excess is also harmful to joints and interferes with successful surgery. Three or more servings of alcohol per day increases the risk of infections, bleeding and heart problems after surgery.
-
Stress Management and Proper Nutrition
Stress management and proper nutrition are healthy practices regardless of hip dysplasia. Mindfulness training and medication techniques can help decrease stress and help muscle relaxation.
There is growing interest in the role of Vitamin D supplementation and anti-inflammatory diets in the management of joint pain. However, the benefits for osteoarthritis caused by hip dysplasia is uncertain compared to inflammatory joint problems such as Rheumatoid Arthritis. The Arthritis Foundation has provided some tips for an anti-inflammatory diet that may help decrease pain which you can learn more about by clicking this link.
Heat therapy: Heating pads can help tense muscles relax. Surface heat may also help relieve pain temporarily by providing skin sensations that are more pleasant than joint pain. However, there is little likelihood that surface heat can improve deep circulation to the hip or change the underlying problem of the bone alignment.
-
Summary of Lifestyle Modifications
Except for weight loss and activity restriction, there are few lifestyle modifications that can slow the process of joint deterioration that results from hip dysplasia. Unfortunately, the underlying problem of hip dysplasia is that the bones are not supporting the joint surface adequately. This causes excessive pressure in areas that wear out faster unless the bones are re-aligned or replaced surgically.
Complementary and Alternative Treatments
There are no known alternative treatments to prevent or cure osteoarthritis. Some people do experience temporary pain relief from symptoms when using alternative treatments, though studies have not shown evidence that this changes the long-term outcome of osteoarthritis.
Acupuncture
Acupuncture is sometimes tried for pain relief. Acupuncture is a traditional Asian practice in which small needles are inserted into the patient and manipulated by the practitioner. The theory of treatment is to improve the flow of energy throughout the body however there is no evidence to support this mechanism.
In 2009, the British Medical Journal published a review of thirteen studies of acupuncture that concluded there was little difference between real, sham, or no acupuncture for relief of pain. Those who report pain relief may be experiencing a placebo effect.
Click Here to View the Article
Avocado-Soybean Unsaponifiables (ASUs)
ASUs are supplements made from a specific type of oil from avocados and soybeans. ASU supplements are thought to slow down cartilage wear and to encourage the growth of healthy cartilage in hip and knee joints.
The oil in the supplements is more concentrated than what is consumed when eating avocados and soybeans. There is some evidence that ASUs may relieve symptoms of arthritis, but the effect may be short term.
Click Here to View the Article
Ginger
Ginger is an edible root often used in cooking as a seasoning. In the context of alternative medicine, ginger is sometimes recommended to settle an upset stomach or to reduce inflammation and its resulting pain. Ginger can be purchased as a supplement, or ginger can be made into a tea.
Ginger contains compounds called gingerols that have anti-inflammatory properties. There is some evidence that ginger has a moderate pain relieving effect for osteoarthritis.
(Caution) Ginger might interfere with some blood-thinning medications. So if you are taking a blood thinner, check with your doctor before taking ginger supplements. Side effects from ginger supplements can include heartburn or diarrhea.
Glucosamine and Chondroitin
Randomized controlled studies have shown that these supplements do not promote the growth of cartilage or improve joint health. It is still possible to buy these supplements, but they will not improve the health of your hip joint.
(Caution) People who are allergic to shellfish should not take glucosamine. Glucosamine and chondroitin can interfere with blood-thinning medicines.
Tai Chi and Yoga
Tai Chi and yoga are traditional disciplines with movements than can help promote strength, flexibility, and balance. Staying active is good for you as long as you do not push your joints to the point that you are in pain or you get injured.
Look for teachers who are willing to work with any limitations that you may have. Some experienced teachers can suggest ways to modify exercises so that they are less strenuous.
(Caution) Though these exercises can improve your muscle strength, posture, and overall health, they cannot change the bone structure of your hip joint.
Other Herbal Remedies
Numerous herbal remedies have shown anti-inflammatory properties including Curcumin, Boswellia Extract, Fish Oils, UC-II, Resveratrol, and more. For more information about alternative medicines, including studies, see the National Center for Complementary and Alternative Medicine at the National Institutes of Health by clicking here or the Cochrane Reviews by clicking here. The Cochrane Collaboration is an independent organization that reviews primary research in health care.
Physical Therapy
Movements of the hip and gentle stretching exercises are recommended because motion may help lubricate and nourish the joint surfaces. Try to maintain hip motion in all directions unless there is pinching in one particular position. Stretching exercises can be performed to move your leg away from your body in the lying position and in the sitting position. Also gently roll your legs in and then out as far as possible to stretch hip rotation. When lying down, pull one knee to your chest while the other leg is lying as flat as possible on the floor, then repeat with the opposite knee. All stretches should be held for 15-30 seconds in the most stretched position. Stretching for as little as 10 minutes a day can make a big difference in flexibility.
When working on hip strengthening exercises concentrate on hip abduction (moving your leg, at the hip, out to the side, away from the body) and external rotation (rotation of your hip away from the body)
Examples of Hip Abduction exercises


If you have a leg length discrepancy, a heel lift may be added to your shoe to reduce pain and help with your walking pattern. A physician’s prescription may be required for an orthotist to appropriately prescribe an orthotic. The Physical Therapist can then manage the muscle strengthening, walking pattern, and home program for the patient.
If you have a leg length discrepancy, an insole can be inserted in your shoe or a heel lift may be added to your shoe. Up to 3/8 inch can usually be placed inside a shoe without any problem. When more is needed you should probably obtain a prescription from a physician to have the lift added to the heel of your shoe. A shoe lift occasionally helps reduce pain and improve walking pattern. Other everyday recommendations would include taking the elevator to avoid using stairs and using ice after a busy day to help reduce pain and possibly allow you to better manage your symptoms.
As a general rule, heat is preferred before activities and ice afterwards (like a warming up and cooling down a race horse), however, heat in the evening helps some people because heat helps muscles relax and increases blood flow to the area. Cold is always used to reduce swelling for the first few hours after a fresh injury, but there isn’t a right or wrong answer about heat or cold for pain relief for arthritis. Other everyday recommendations would include taking the elevator to avoid using stairs and using ice after a busy day to help reduce pain and possibly allow you to better manage your symptoms. Depending on the level of dysplasia this may require one or two visits with a local Physical Therapist to teach you the correct way to exercise without causing damage to your hip.
Pregnancy After Hip Dysplasia
Normal childbirth is a frequent concern for women who have had surgery for hip dysplasia. Fortunately, the need for Cesearean section is rarely influenced by hip dysplasia or hip dysplasia surgery.
Your obstetrician can measure the size of the pelvis prior to childbirth to help determine possible need for Cesearean section. Sometimes hip motion is restricted and this can lead to Cesearean section if the hip doesn’t have enough movement to allow normal childbirth.
Hip dysplasia by itself is not associated with increased difficulty with normal delivery. With hip dysplasia the socket itself is shallow, but the internal borders of the pelvis have normal size and shape. HIp surgery during childhood rarely causes problems with pregnancy later in life. Surgery like open reduction, or femoral osteotomy would not change the shape of the pelvis and the pelvis is normal size and shape for most women with hip dysplasia.
Even pelvic surgery during childhood has so much remodeling capacity that any surgery prior to the age of six years should smooth out and accommodate normal pregnancy and childbirth. When pelvic surgery has been performed after the age of six years, the pelvic bones can become slilghtly distorted and cause problems with childbirth. In these cases it may be helpful to know what kind of surgery was performed on the pelvis. The Ganz Osteotomy (also called the PAO) is a commonly performed bone surgery in adolescents and adults with painful hip dysplasia. The PAO does not restrict pelvic diameter. The less common types of pelvic surgery that might cause concern are the Steel, Chiari, Sutherland, and Salter osteotomies when these have been performed on both hips or after the age of six years. The Salter, Dega, and others are used in young children and shouldn’t be problematic.
In summary, it is very uncommon for hip dysplasia or hip dysplasia surgery to be a problem for delivery. Of course, your obstetrician will help you decide whether you might need to plan for a Cesearean section after you become pregnant. Also, we know you will remember to have the pediatrician double-check your child because there is a slightly increased risk that your children may have loose hips that can become dysplastic.
Sports and Activities
Exercise and strengthening is recommended to maintain muscle balance and cardiovascular health as long as there isn’t too much load put on the hip joint. Running and impact sports are not recommended for people with hip dysplasia. Sports like golf and bowling are not likely to add damage the hip but there may be pain in certain positions.
Try to maintain upper body and trunk strength along with normal tone and strength in the hip and leg muscles. Also, weight management, and a modest activity level are helpful to protect the hip and preserve as much function as possible.
For cardiovascular fitness, we recommend upper body activities and trunk exercises instead of running, stair-climbing, or impact exercises. Swimming can emphasize upper body activities while the body weight is supported. Other activities like rowing, cycling, or tennis may be possible in moderation, but these can be difficult for arthritic hips because of stiffness and muscle actions that place loads across the hip joints.
Movements of the hip and gentle stretching exercises are recommended because motion may help lubricate and nourish the joint surfaces. Walking with a cane in the hand opposite the sore hip can also provide some physical activity in later stages of painful hip dysplasia. Depending on the level of dysplasia, you may benefit from one or two visits with a local Physical Therapist to teach you the correct way to exercise without causing damage to your hip.
Work Related Concerns
Twenty to forty percent of patients with hip dysplasia will eventually develop osteoarthritis. Many will need surgical intervention to improve their daily quality of live. Along with this physical burden, this can also become a financial burden. It is estimated that over 46 million adults in the USA have osteoarthritis. According to American Journal of Managed Care, the total medical expenditures for patients with arthritis are as high as 89.1billion dollars per year. They further stated (from 1997-2003) that 9.4 % of patients with osteoarthritis were unable to acquire jobs as a result of their illness compared to non-arthritic people. This resulted in an annual wage loss of approximately $3600-$4500 per person.
The number of hip replacement surgeries has increased rapidly as our population has aged in recent years. It is anticipated that the yearly number of total hip replacement surgeries will be approximately 572,000 by 2030. The average age of total hip replacement is around 68 years of age. According to Mobasheri et al., 15% of hip replacements are done in people of working age. In their study, 49 of 51 patients who were employed prior to surgical intervention returned to work after having a hip replacement. The authors further stated that 13 out of 30 patients who were not employed prior to a hip replacement were able to find some form of employment after their operation. The average return to work for the patients undergoing total hip replacement averaged 10.5 weeks.
During rehabilitation for total hip replacement and other hip surgeries there is usually a need to strengthen the hip muscles especially the hip abductors (the muscles that spread the legs appart). Weight loss is always recommended to reduce the strain on the hip joint. While at work, a comfortable seated position is usually recommended in the early stages of healing. However, prolonged sitting can cause recently operated joints to become stiffer. Periodic 5-10 minute walks may allow the recovering patient to keep motion in their joints. According to the American Academy of Orthopedic Surgeons, climbing stairs should be limited until your doctor says that healing and strengthening are adequate for such activities. When climbing stairs it is recommended to step up with the unaffected leg first. Then the affected leg is brought to the same step instead of to the step above. This is slower than normal stair-climbing, but it puts less strain on the painful or operated hip. If you are using a cane or crutches then bring them up to the same step before proceeding. The process is then reversed to go down stairs.
Before any surgery it is always a good idea to ask your orthopedic surgeon about postoperative activities and limitations following surgery.