
This surgery means the hip joint is opened up to clear out any tissue(s) that is keeping the head of the femur (the ball) from going back into the acetabulum (the socket). There are two general approaches to this procedure:
Medial Approach
This approach is normally successful for children less than one year of age. This procedure starts through a small incision in the groin (medial to the hip). This is a limited surgical approach that allows the joint to be cleared so the hip can be aligned into the socket.
This method is typically used when a closed reduction is unsuccessful and the arthrogram shows something in the joint that’s keeping the hip out of the socket.
This method cannot correct any underlying problems in bone structure.
A spica cast is normally needed for a few months to keep the hip aligned, while it is growing and becoming more stable.
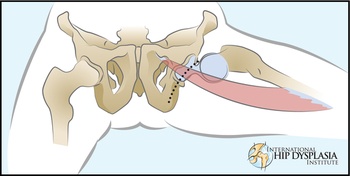
Anterior Approach
The anterior approach to the hip joint is used when the ligaments around the hip need to be repaired and tightened after the hip is cleaned out and aligned. This is used after the age of 12 months when surgery is needed, or for more severe hip dislocations.
Reshaping the hip socket can also be done through this approach.

What to expect after surgery for open reduction of dislocated hips
This usually depends on three things:
- The type of surgery
- The method of immobilization after surgery
- Post-operative management that has worked best for your surgeon
Here are some categories with general points that you might want to discuss with your surgeon
Open reduction surgery without bone surgery
Generally, this type of repair is held together with strong internal sutures that do not need to be removed. However, more time is often required for the ligaments to heal. Children younger than one year may be in a cast for as long as three months followed by brace treatment in order for the hip to become stable and for the bones to remodel to the new hip position.
Open reduction surgery without bone surgery after the age of 12 to 15 months generally requires bone reshaping to accelerate the process.
Open reduction surgery with pelvic and/or femoral osteotomy
This type of repair holds the ligaments together with strong internal sutures but the bones need to be re-shaped so smooth pins or metal plates and screws are used to hold the bones in position while they heal into their new shape. A hip spica cast is generally used for six to eight weeks after surgery to help hold the hip in the socket while the ligaments and bones are healing.
The pins, plates, and screws need to be removed at a second procedure. The second procedure is quick but needs general anesthesia in the operating room. This can be performed in almost all cases as outpatient surgery so the child goes home the same day. A cast is not needed after removal of metal implants. Pain is minor and can be managed by numbing medicine that is injected at the time of surgery combined with Tylenol and codeine syrup for 24-48 hours.
What to look for
In the hospital
- During the first few days after surgery the private areas may be swollen and black-and-blue from the surgery. This will resolve but may create problems with placing the diaper. If the swelling is pressing against the edges of the cast or causing diapering problems, show the area to your doctor and ask for his/her opinion.
- Moving, or picking up your child in the cast may cause discomfort, but the cast is protecting the hip so there’s no need to worry about doing something wrong.
- Do all you can to keep the cast clean and dry while in the hospital. Not all nurses are familiar with spica cast care and they may be more focused on bigger concerns such as circulation, hydration, infections, pain relief, and recovery from anesthesia.
- Cast technicians are available in the hospital to make adjustments to the cast if the edges are sharp, or there isn’t enough room for diapers or bodily functions. It’s best to try to get the cast as perfect as possible before leaving the hospital. Show any areas of concern to your nurse or your doctor.
Tips for spica cast care.
These can be found elsewhere on this website:
One item that can help smooth and soften the edges of the cast is Moleskin tape that can be purchased at most local pharmacies or online.
Skin problems and infection
These are the most common concerns after surgery. Skin problems can be kept to a minimum with careful attention to padding the edges of the cast, and keeping the cast as dry as possible. A hair dryer on cool setting can help skin stay dry and also decreases itching from moisture.
Low fever is very common in the first few days after surgery and is rarely a sign of infection. Fluids and acetaminophen can help control this. However, after the first few days, any fever greater than 37°C, or 101°F, should be reported to the nurse or doctor who is caring for your child. Infections may also have a foul smell that is different from stale urine. Sometimes the bandage holds blood that can stay moist and cause of bad odors, but bad odors need to be reported to your doctor. Bandages on the skin rarely cause problems by themselves because the skin incision sticks together very quickly and forms a protective scab to resist infection.
Cast Removal
When the cast is removed, your child will probably be frightened and uncomfortable because of the change in feeling without the cast. Their joints and muscles have been in the same position for weeks so the first movements will be uncomfortable. Imagine what you might feel like if you were sitting in the back seat of a small car for six weeks and then you were asked to get out. You wouldn’t want to move very fast and neither will your child. As much as possible, support the legs in the same position as the cast until you can place the child in a tub filled with warm water. The water will provide support for gentle movement that the child can do without help from adults.
In the doctors’ office, try to keep your child from scratching the itchy skin because that may increase the skin problems. It will be helpful to be prepared with some warm wash cloths ready to soothe the dirty and sometimes crusted skin. Some children will also have a heat rash, or red irritated skin. A warm wash cloth can soothe this until reaching home for a warm bath. Avoid oily creams that may clog the skin. A simple remedy for heat rash is baking soda. A soothing paste for the skin can be made by mixing two tablespoons of baking soda with a tablespoon of water. Also a cup of baking soda can be put into the bath water, or washcloths may be dipped into a quart of water with two or three tablespoons of baking soda in the water. Anhydrous lanolin is also soothing and easily removed with water. Even though the skin may look bad initially, almost all rashes will clear by themselves in a few days after the cast is removed.
Weeks and months after surgery
Often a brace is used after the cast is removed in order to support the hip joint for several more weeks and sometimes even longer at night. It is important to maintain the hip in the most stable position to avoid re-dislocation even after the cast is removed. There should be no rush to restore movement to the hip joint. This will occur naturally and may take weeks or months.
Children may not walk for weeks after cast removal and this is OK too. It is likely that the child will crawl before pulling up to stand. Then, the child may cruise by holding onto furniture before learning to walk again. This may take weeks, and the child will often walk with a limp for months. This is all natural because the hip joint has been rearranged, and tightened up surgically. It will take some time for the child to learn how to use his or her new hip joint.
Think of a professional athlete who tears a knee ligament and requires surgery to repair the damage. That athlete will not fully recover for 8 to 12 months even when they are being encouraged by a physical therapist or personal trainer. Fortunately children rarely need a therapist to teach them to exercise because children want to climb, run, jump, squat, and do all sorts of things to test their muscles and joints. With normal attempts at childhood activity, it is reasonable to expect your child to take a year to recover full strength and mobility after major hip surgery. Your child may trip and fall more than other children who have not required surgery, but that is normal as they test themselves and try to do more. If they haven’t recovered as much as your doctor expected, then a physical therapist may be able to help.
The healing process inside the hip joint is similar to the healing process of the skin. At first the scar may be red, firm and raised. With time, the scar will soften and become less visible. The flexibility will gradually return as the scar matures. When the scar is fully mature it will be soft, flexible and less visible. That also suggests that the internal healing is complete and the hip joint has probably recovered as much motion as possible.
In summary, the recovery process after hip dislocation surgery is long. There is no need to rush the process because children have amazing abilities to recover. A year or longer is needed for most children.